



The Migraine Mystery – Explained
Medical researchers estimate that at least 20% of the population suffer weekly, and even daily, from some kind of headache or common migraine. Migraines occur more often in women than men. Approximately 25% of women and 8% of men suffer from migraines at some time in their lives.

Migraines are different from other headaches and can occur with additional symptoms such as nausea, vomiting, fatigue, and sensitivity to light. A migraine episode can last hours, days, or weeks, leaving the sufferer virtually disabled for that time. A migraine attack can be induced by various triggers, including bright light, certain food items, and alcohol. Uncontrollable triggers can include food allergies, changes in the weather, and menstrual cycles. Migraines can be caused by psychological factors, although stress and depression can also result as a consequence of the debilitating and chronic migraine pain.
There are many types of migraine 'designations' and 'names' that the medical community has given this common problem, such as primary, secondary, hemiplegic, ocular, intractable, aura, silent, abdominal, vestibular, etc. The reason that you have so many migraine categories is actually due to the lack of proper diagnosis and missing knowledge about the actual cause of migraines. The rest of this page will explain what causes migraines and headaches and why most people are being misdiagnosed and treated ineffectively. Modern medical therapies and medications are a multi-billion-dollar industry that lacks results.
Can Drugs Relieve or Control Migraine Pain?
All treatments for migraine have the same goals in common: halt, or at least reduce the excruciating pain and minimize the other significant symptoms, such as nausea and vomiting. Today’s medical treatment methods employ a variety of different strategies to control and ease the pain. Migraine treatment usually falls into two categories: medications that stop an attack (acute treatments) and medications that prevent attacks (preventive treatments). The most commonly used today include: 🟢 Acute (Rescue) Medications are taken when a migraine starts: Triptans (first-line choice for moderate to severe migraines) Examples: Sumatriptan, Rizatriptan → Targets serotonin receptors to reduce inflammation and pain NSAIDs (nonsteroidal anti-inflammatory drugs) Examples: Ibuprofen, Naproxen → Often used for mild to moderate migraines Gepants (newer CGRP blockers for acute use) Examples: Ubrogepant, Rimegepant → Alternative for people who can’t take triptans Ditans Example: Lasmiditan → Designed for patients with cardiovascular risks (no vasoconstriction) 🔵 Preventive (Preventative) Medications are taken regularly to supposedly reduce frequency and severity: CGRP monoclonal antibodies (very commonly used today) Examples: Erenumab, Fremanezumab, Galcanezumab → Specifically "designed" for migraine prevention Beta blockers Examples: Propranolol, Metoprolol → Originally for blood pressure, widely used for prevention Anticonvulsants Examples: Topiramate, Valproate → Try to stabilize nerve activity Antidepressants Example: Amitriptyline → When migraines overlap with sleep or mood issues Overuse of acute meds has been shown to lead to medication-overuse headaches! Many patients use a combination of acute + preventive therapies
Can Drugs Provide Long Term Solutions?
Many treatments can reduce migraine frequency and severity over time. Preventive therapies—especially newer CGRP-targeting drugs like Erenumab or Galcanezumab—were specifically designed based on migraine biology. Clinical studies and real-world use show they can reduce monthly migraine days for many patients, but efficacy is less than 50%. For patients who experience constant pain, these drugs do not solve the problem. Acute medications can be effective when used correctly. Drugs like Sumatriptan can interrupt the migraine process if taken early enough. For many people, they reliably stop attacks. However, they do not provide a long-term resolution of the problem. Most of these migraine medications manage symptoms and can reduce frequency but don’t cure the actual cause or condition. Improper or excessive use can worsen headaches in some patients. We find the cause of the migraine and can actually provide you with a guarantee of treatment.
Genetic Factors
Headaches can start between the ages of 10 and 46, and can have some genetic components. The genetic factors are due to skeletal imbalance problems that are passed on from generation to generation. It is these skeletal imbalance problems that must be diagnosed and treated in order to eliminate the chronic pain.
Standard Diagnosis
Migraine headache may be diagnosed by your family doctor based on your symptoms. Your doctor will take a detailed history to make sure that your headaches are not due to sinus inflammation, or a more serious underlying brain disorder. During the physical exam, your doctor will probably not find anything wrong with you.
Your doctor may refer you to a neurologist and possibly order an MRI or CT scan to rule out other causes of headache, such as sinus inflammation or a brain mass. In the case of a complicated migraine, an EEG may be needed to exclude seizures. Rarely, a lumbar puncture (spinal tap) might be performed to rule out bacterial or viral infections. These tests are recommended by your doctor and us for all chronic head pain patients!
Stroke is an extremely rare complication from severe migraines. This risk may be due to prolonged narrowing of the blood vessels, limiting blood flow to parts of the brain for an extended period of time.
Migraine headache patients are normally told that it’s just stress or a sinus problem or perhaps some residual, lingering effect of an accident we had years ago. Sadly, a sizable number of these inadequately diagnosed patients are recommended to use popular pain medications, which do nothing to address the root causes of pain.
Most migraine sufferers go from doctor to doctor looking for the definitive treatment that will permanently resolve their pain. Each new physician, or therapist, claims expertise in pain management and proceeds to treat it accordingly. Often, the results are temporary.
Based on our decades of experiences and treating tens of thousands of chronic head pain sufferers we have found that nearly all headache practitioners fail to recognize and address the most critical problem: craniomandibular dysfunction.
How We Diagnose Migraine Causes at our Office
So, how do you find the correct diagnosis and the proper treatment for your migraine problem? Fortunately, today’s modern craniofacial pain treatments are curing chronic headaches, migraines, and facial pain with nearly 100% success rate. The explanation for your migraine problems and the cause behind your symptoms is as follows.
Research has undeniably established the association between intense chronic muscle contraction and chronic pain, especially in your head. When any muscles become overused, pain begins to develop in those muscles and associated structures. The bulk of this dysfunctional muscular activity starts to eventually damage any neighboring joints and ligaments. When joints become damaged muscles try to protect them by splinting themselves into even more activity. An endless cycle ensues and pain worsens. 95% of headaches and migraines have an underlying factor: damage to the TMJ (jaw joint) and trigeminal nerve caused by overactive jaw muscle activity or genetic skeletal imbalance factors. Many times this damage goes unnoticed and undiagnosed by your physician and your dentist. Eventually the muscle dysfunction, trigeminal neuritis, and joint damage can lead to debilitating pain, sensitivity to light, and all of the other symptoms of the common migraine.
Most common headaches start out as simple muscle tension problems. Remember that bad day at work? You probably clenched your teeth all day and assumed a “tense” postural position while working. For a majority of us, a couple of Advils take away that sporadic problem. Unfortunately, for the migraine sufferer the Advils stopped working a long time ago. The reason is simple: the migraine patient has an undiagnosed skull imbalance or jaw joint problem which worsens over time. This is especially true when they clench or grind their teeth or may have been born with an unstable or deficient bite. This problem can be the result of genetics or long-term wear and tear. The patient who had braces to correct crooked teeth has the same possible jaw joint damage that a person who wears down their jaw joints due to constant clenching and grinding. The common denominator is that the migraine patient has developed some abnormal muscle function and usually extensive damage to the jaw joint that has been neglected and undiagnosed. These two problems lead to worsening muscle function, abnormal trigeminal nerve conduction, and blood flow alteration inside of the brain. Research has shown that the jaw muscles of a migraine patient can be in a constant state of tension (or contraction) while the trigeminal nerve exhibits abnormal excitation. Other factors begin to develop as a result, which can cause the entire nervous system to become unbalanced.
Other factors begin to develop as a result of the constant state of tension. The nervous system has 3 parts: the voluntary one, which you control, and the 2 involuntary parts that you cannot control (sympathetic, which gets you into high gear and parasympathetic, which allows you to heal). The sympathetic nervous system begins to overwork itself in patients with abnormal muscle function. Increased input to the muscles from the sympathetic nervous system further increases the tension and contraction of the muscles. It’s a 'silent' action, one that is not readily observed clinically.
The sympathetic nervous system subsequently begins to overwork itself. Increased input to the muscles from the sympathetic nervous system increases the tension and contraction of the muscles. At the same time, lack of parasympathetic nervous system activity can cause metabolic, digestive, and cardiovascular problems as the body cannot properly heal due to lack of parasympathetic nervous system function.
Nervous System Overstimulation
People with chronic pain feel as though their bodies are burning up. This is a normal response to the pain being caused by the nervous system. Pain eventually leads to loss of sleep, and prevents the nervous system from coming into balance. The sympathetic nervous system (the accelerator) does not shut down and our bodies get depleted. We feel tired, irritated, nervous, depressed, and angry. The parasympathetic nervous system requires time to replenish the body with the hormones and nutrients that it needs. The sympathetic system overtaxes the system and thereby causes the parasympathetic system to function inefficiently by not allowing it to turn on. Health problems kick in.
Is Your Migraine Pain Caused by Stress or Tension?
Stress — Daytime and Nighttime
It’s during certain stressful parts of the day that we clench or grind and cause muscular damage. At night, the stress can continue. During sleep even the slightest touching of the teeth requires contraction of the temporalis and masseter muscles. You can’t put your teeth together without contracting these two powerful muscles. Stress and anxiety can cause severe clenching.
As a basic rule of Mother Nature, your teeth should not touch more than a few hundred times per day! This allowance is for when you chew finer foods like spinach or lettuce. Otherwise, your teeth are designed to mesh food without having to crunch themselves together! It’s a good bet that your teeth are probably touching right now as you read this page. Forcing your teeth to touch requires contraction of the temporalis and masseter muscles. Continual contraction of these closing muscles creates a dysfunctional state as described above. This problem may not be painful until later in life. It takes time to damage the teeth and jaw joints and associated structures. This endpoint usually happens when the jaw joint wears out and all surrounding tissues go into a “silent” dysfunction due to the damage. This 'silent problem' is called a migraine.
Stress, Tension, or Genetics?
Please remember that the migraine patient can also have a genetic problem of jaw imbalance that they inherited from a parent. A jaw imbalance causes faster and more rapid wear and tear of the joint, especially when coupled with abnormal muscle activity. Many times, this is a slow process that begins during childhood and continues without the person being aware.
If the sufferer has a genetic component of jaw imbalance problems, then the body senses this inherent dysfunction as damage to the body and tries to protect it by sending even more muscles into spasms. The muscle function and joint damage is not readily diagnosed or observed by a majority of doctors.
Understanding the Muscular System Role in Migraines
The way your teeth, jaw, skull, and neck work together plays an important role in how your body experiences pain. When this system is out of balance—especially around the Temporomandibular joint—it can place excessive strain on muscles and irritate nearby nerves. Over time, this added stress may contribute to a range of symptoms, including headaches, jaw pain, facial pain, and neck discomfort. In some individuals, it can also act as a trigger that worsens conditions like Migraine, as well as symptoms such as Tinnitus and Vertigo. The structural and muscular imbalances are often an overlooked piece of the puzzle. By identifying and correcting these imbalances it is possible to reduce strain on the nervous system, improve function, and help patients experience meaningful relief—especially when this approach is combined with a comprehensive understanding of how the brain and body process pain.
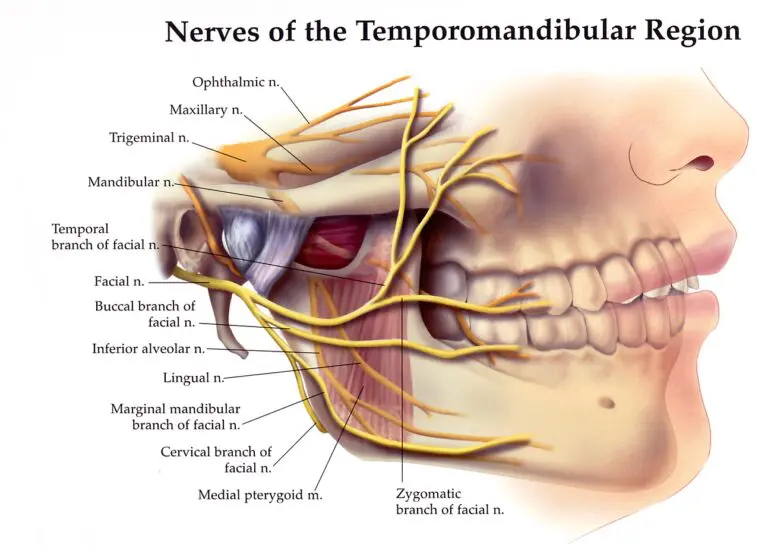
Trigeminal Complex
The Trigeminal nerve is the primary nerve that carries sensory information—including pain—from much of the face, teeth, jaw, and parts of the head to the central nervous system. Because of its extensive reach, irritation or dysfunction in areas it serves—such as the jaw muscles or teeth—can contribute to head and facial pain. In people who are already susceptible, input from trigeminal pathways can trigger or worsen migraines and certain types of headaches. It can also play a role in conditions like facial pain, jaw disorders, vertigo, dizziness, ear pain, and tinnitus.
Contemporary research indicates there is general agreement in the medical community that the Trigeminovascular system (trigeminal nerve + associated blood vessels) plays a key role in migraine. The Trigeminal nerve carries pain signals from the face, meninges, and blood vessels to the brain. Activation of this system is linked to release of molecules like CGRP, which is why newer drugs target that pathway. Treating symptoms with medications unfortunately does not resolve the real cause of the problem.
The Trigeminal nerve is a major pain pathway in the head and is central to migraine. In migraine, the Trigeminovascular system becomes activated. Trigeminal fibers release neuropeptides (like CGRP) around the meninges, which promotes inflammation and sensitizes pain pathways. Jaw/TMJ issues—at the Temporomandibular joint and surrounding muscles—can trigger and amplify headaches because they share trigeminal innervation. The medical community considers Migraine as a neurovascular disorder, with brain network excitability leading and vascular changes following. Research is never aimed at finding the true cause since that would not drive the stock price of Big Pharma. Treating symptoms is huge profits. Solving the real problem is not financially rewarding.
The trigeminal nerve plays a central role in migraine because it connects directly to the brainstem and helps carry pain signals from the head and face to the brain. When this system becomes overly sensitive—as it often does in headache sufferers—it can amplify pain signals and make the nervous system more reactive to everyday stimuli. In migraine patients, the nervous system doesn’t regulate sensory input as efficiently as it should. Instead of filtering and calming incoming signals, the brain can become more easily overstimulated. This heightened sensitivity is part of what leads to recurring headaches, facial pain, and increased response to triggers like stress, muscle tension, or poor sleep. Neurotransmitters such as serotonin also play an important role in this process. Rather than acting as “fuel,” serotonin helps regulate how pain signals are processed and how blood vessels and nerves respond during a migraine. When these systems are out of balance, it can contribute to the onset and persistence of symptoms. Over time, repeated activation of these pain pathways can make the nervous system more prone to future episodes—a process often referred to as sensitization. This is why headaches can become more frequent or intense if the underlying patterns aren’t addressed. Jaw tension or muscle dysfunction contributes to this cycle in the majority of migraine patients. It is important to understand the complex interaction between the brain, nerves, teeth, jaws, jaw joint, muscles, ligaments, blood vessels, and sensory processing systems.
How Serotonin Affects Your Nervous System
Neurotransmitters like Serotonin play an important role in how your brain regulates pain, mood, and sensory input. In conditions like Migraine and chronic headaches, these systems can become imbalanced—making the nervous system more sensitive and reactive. Over time, this heightened sensitivity can affect many areas of daily life, including focus, energy, mood, sleep, and overall well-being. That’s why head pain is often more than “just a headache”—it can impact how you function day to day. Many commonly prescribed medications—such as Sertraline (Zoloft), Fluoxetine (Prozac), or Sumatriptan (Imitrex)—are designed to help regulate these pathways and reduce symptoms. For some patients, they can be helpful in improving quality of life. But for how long? Medication alone doesn’t address why the nervous system became dysregulated in the first place. Factors like muscle tension, jaw dysfunction, poor sleep, stress, and structural imbalances can continue to place strain on the system. Medication treats symptoms, not cause. That’s why a comprehensive approach is needed—one that looks beyond symptom control to identify and correct contributing factors. By improving how the muscles, joints, and nervous system work together, it’s often possible to reduce stress on the body and support more lasting relief.
Function Can Affect Structure
It is critical to realize that human beings use their lower jaw over 5,000 times a day. Think about what would happen if you tried to ride 1,000 miles on a bicycle that had missing spokes.
Your lower jaw is one of the most active joints in your body—used thousands of times every day for speaking, chewing, and even subtle movements you don’t notice. When this system isn’t functioning properly, the effects can add up quickly. The jaw, head, and neck are closely connected through muscles and the Trigeminal nerve, a major pathway that carries sensation and pain signals to the brain. When there is ongoing strain—whether from clenching, grinding, bite imbalance, or muscle overuse—the system can become overloaded. This constant stress can lead to muscle fatigue, joint irritation in the Temporomandibular joint, and increased sensitivity in the nervous system. Over time, that heightened sensitivity can act as a trigger—contributing to recurring headaches, facial pain, and even worsening symptoms like Migraine. Think of it like driving a car with poor alignment. You can keep driving, but the longer it goes uncorrected, the more strain builds—and the more problems begin to surface. The key is to manage symptoms, identifying the cause, and correct the underlying sources of stress on the system. By improving how the jaw, muscles, and nervous system work together, it’s often possible to reduce that overload and help the body function more comfortably and efficiently.
Vascular System Involvement
The trigeminal nerve is a key pathway for head and facial pain and it is directly linked to what we call craniomandibular dysfunction of the jaws.
Many patients may feel a migraine on only one side or in their eye or top of head. The reason for this can often be diagnosed by which side the jaw joint is more damaged or where the muscle activity is more chronic. For example, patients who have lost teeth on their right side will experience more pain there due to loss of support and abnormal muscle and nerve activity on that side. The trigeminal nerve on that side is more affected.
A full head and neck anatomy examination is also important. The following video shows our full examination protocols:
COMMON MIGRAINE TERMS…And misconceptions
If you have been diagnosed with migraine you may have heard some other common terms that the medical community has coined for this problem.
Ataxia. This means you have trouble using your muscles. It leads to lack of coordination and can make it hard to walk. It usually comes with a type called migraine with brainstem aura. It can be a result of neurological disease and may not be associated with the causes explained on this website.
Aura: Changes in vision or sensation before or with a migraine. Common sensations can include flickering lights, spots, or lines, or a loss of vision. Sometimes the person may experience numbness or tingling in other parts of the body. Speech may also be affected (Dysphasia). Sensory Aura can also be experienced in terms of tingling face, mouth, arms, or even legs.
Cause: The ophthalmic division of the trigeminal nerve is in dysfunction and normally caused by a damaged jaw joint or abnormal jaw and neck muscle function.
Cutaneous allodynia: This is when touching your skin becomes painful. During a migraine, it might hurt to put in contacts, shave, or brush your hair. Trigeminal neuralgia can cause such symptoms.
Cause: The trigeminal nerve is in a state of severe irritation normally due to damage of the TMJ!
Diplopia: Double vision.
Cause: Reduction of blood flow to the ophthalmic blood vessels caused by strained muscles and constriction of blood vessels!
Hemiplegic migraine: One-sided pain commonly mistaken for a stroke or epilepsy. It is important to have a brain MRI to rule out stroke or other diseases.
Cause: Damage to the jaw joint on that side of the head!
Hyperosmia: Hyper-sensitive or change of smell.
Cause: Hypersensitivity of the trigeminal nerve 2nd division caused by compression of the TMJ!
Menstrual migraine: If you only get them 2 days before your period or in the first 3 days after it starts your problem may be hormone related. Otherwise, there is a high probability that your hormonal shift is causing an increase in already irritated facial and trigeminal nerves.
Migraine prodrome: This phase of the migraine cycle happens 24 to 48 hours before a headache starts. You might notice symptoms like crankiness and mood swings, food cravings, constipation, and neck stiffness. You might notice that you yawn a lot.
Cause: Most likely stress induced by clenching and hyperactivity of jaw muscles along with a jaw joint that is already damaged
Ocular migraine: Affects your sight, like blind spots, zigzag lines, seeing stars, and even vision loss (scotoma).
Cause: Compression of the 2nd division of the trigeminal nerve due to a damaged TMJ.
Phonophobia: Sensitive to sound during a headache.
Cause: Compression of the 2nd division of the trigeminal nerve due to a damaged TMJ. Ear structures are under heavy stress caused by the TMJ.
Photosensitivity/Photophobia: Being around sunlight or artificial light may make you feel even more uncomfortable.
Cause: Compression of the 2nd division of the trigeminal nerve due to a damaged TMJ.
Dizziness/Vertigo: The sense that you’re spinning (or the world around you is spinning) when you’re really not. Dizziness may involve a sense of lightheadedness or trouble keeping your balance.
Cause: Compression of all 3 divisions of the trigeminal nerve due to a damaged TMJ and abnormal pressure of the ear structures.
To learn more, contact us today! Solve your pain in 6-8 months or we’ll give you your money back.